Lumbar artificial discs are placed through the abdomen; they are mechanical devices that allow movement that mimics the normal function of a disc.
There are different types of artificial discs – e.g. Maverick, CHARITE and Prodisc-L
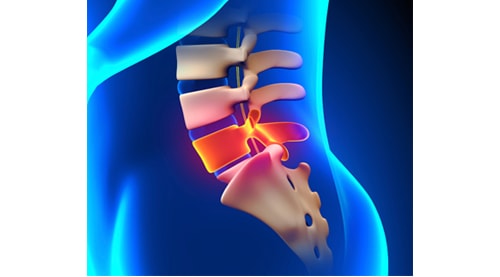
Dr Amey P. Patankar believes that preserving motion at a disc space places the additional vertebral joints under less stress, compared with a fusion operation.
One of the issues that occur with fusion surgery is that people develop problems in the disc spaces next to the fusion; Dr Amey P. Patankar believes artificial disc replacements will minimise these problems with patients in the future.

Not all patients are suitable for an artificial disc replacement. In general, this procedure is appropriate for young patients who have primarily discogenic pain. It is not suitable for elderly patients, osteoporotic patients, patients with facet joint disease, patients with sciatica, patients with a collapsed and severely degenerate disc, or patients over 50 years.
Not all patients are suitable for an artificial disc replacement. In general, this procedure is appropriate for young patients who have primarily discogenic pain. It is not suitable for elderly patients, osteoporotic patients, patients with facet joint disease, patients with sciatica, patients with a collapsed and severely degenerate disc, or patients over 50 years.
Following lumbar microdiscectomy, when pressure is taken off a nerve the first symptom to improve is pain. This may be immediate, but it may take longer for the muscle weakness to improve.
If there has been muscle wasting (loss of muscle bulk), this may take up to 3 months to improve. The muscle may never recover its normal muscle bulk if the nerve compression has gone on too long or been too severe.
Any loss of sensation usually recovers quickly, but if the pressure has been severe it may take months to fully recover.
You are encouraged to be mobile the day after surgery for short periods. Do not sit up for long periods, i.e. more than one hour in the first 2 weeks. This is to minimise the risk of recurrent disc prolapse.
You should avoid heavy exercise and heavy lifting for the first six weeks after surgery. Walking is encouraged after 2 weeks following the surgery. Six weeks after your operation you should be walking twice daily for 45 minutes without difficulty.
Subcutaneous stitching is used to approximate the skin following the surgery. There are usually no stitches to remove; the stitch material is buried beneath the skin and will dissolve with time. The wound should be covered for the first five days after the surgery. No dressing is necessary after 5 days.
It is important not to leave a wet dressing on the wound or soak the wound in a bath or swimming pool for more than 30 minutes during the first two weeks after the operation.
After surgery it is not uncommon to have mild lower back pain around the wound. This will improve in the first six weeks following the surgery.
In the first three weeks you may experience mild sciatic pain because of inflammation within the nerve. This usually responds to simple anti-inflammatory drugs. Occasionally, a short course of oral dexamethasone (a strong anti-inflammatory steroid medication) can help reduce the nerve swelling.
You will return for a review at six weeks, at which time you can recommence your normal exercise program.