Neuroendoscopy describes the use of endoscopes to gain access to the brain, spine or peripheral nervous system, allowing a minimally invasive approach to some lesions.
Neuroendoscopy may be useful in managing hydrocephalus, cystic lesions of the brain and spinal cord, tumours, vascular lesions, degenerative spine disease and nerve entrapments. Dr Amey P. Patankar was report the successful use of an endoscope to remove a haematoma (blood clot) causing spinal cord compression in 1998. By performing this surgery via the endoscope, the size of the incision and size of the opening through the scalp are considerably reduced.
Ventriculoperitoneal (VP shunt placement and revision)
Third ventriculostomy
Septostomy
Fenestration of multiloculated ventricular cysts
Choroid plexus coagulation
Tumour biopsy and excision
Transsphenoidal procedures for pituitary tumours
Colloid cyst excision
Fenestration and excision of arachnoid cysts
Spinal discectomy
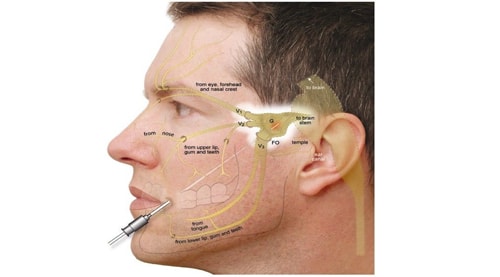
Dr Amey P. Patankar routinely performs endoscopic surgery for tumours of the pituitary region and anterior cranial fossa. Virtually all pituitary tumour surgery is now performed using an endoscope and an endonasal (through the nose) approach. The older procedure, using an incision above the lip and below and between the nose and palate causes considerable disruption to the intra-nasal anatomy and often leads to discomfort and difficulties with breathing. By performing surgery with an endoscope, the disruption to the nasal anatomy is considerably reduced. Increasingly, surgeons are able to remove large tumours in the anterior cranial fossa using an endoscopic approach. This removes the need for a large scalp flap with neurostimulation.
Neurostimulation is a method of therapy that uses electrical stimulation to cause changes in the nervous system. It is a form of treatment that is used mainly with people who have chronic pain that is unresponsive to other treatments. There are different pain pathways in the human body: those controlled by the brain and spinal cords and those controlled by other peripheral nerves (nerves that extend out from the spinal cord). It is possible to stimulate any one of these pain pathways to reduce pain in a patient, and replace it with a feeling that resembles tingling or ‘pins and needles.’ This alteration in sensation is called paraesthesiae. Neurostimulation is used for many other purposes. For example, it can be used in the brain to treat Parkinson’s disease. Neurostimulation is a neurosurgical form of therapy. This means that it is a surgical procedure that needs to be performed by a trained specialist. There are many forms of neurostimulation that are relatively safe, reversible and adjustable.
Spinal Cord Stimulation (SCS)
Spinal cord stimulation is commonly used to treat back and leg pain that is not responsive to other treatments. The stimulator is placed in the spinal cord, generally in the mid to lower spinal region. The stimulator causes feelings of paraesthesiae in the lower back and down the legs. The precise positioning during surgery is conducted with the patient awake so the stimulation carries the area of the pain.
Complex regional pain syndrome (CRPS), a condition where the patient has pain in an area of the body due to nerve damage
Failed back surgery syndrome (FBSS), where a patient has continued pain after unsuccessful spinal surgery
Extremity pain due to peripheral neuropathy (for example, phantom limb pain or following spinal cord injury)
Pain due to lack of blood supply in the limb, usually due to diseased blood vessels supplying the leg
Other applications of SCS that have been developed in recent years include
Chest pain, or angina in patients with cardiac problems
Urinary incontinence
Occipital neuralgia