Lumbar Disc Surgery
There are 4 types of surgery for lumbar disc disease:
Microdiscetomy and nerve root decompression
Lumbar Laminectomy
Lumbar fusion
Lumbar artificial disc replacement (arthroplasty)

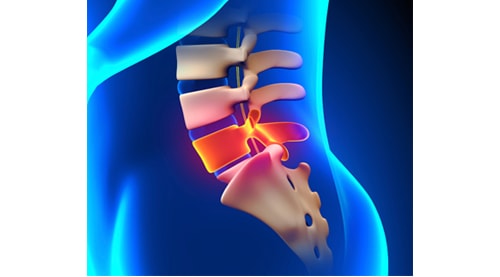
Laminectomies are typically performed to treat spinal stenosis. This the narrowing of the spinal canal that contains the spinal cord and the spinal nerves that arise from the spinal cord. Spinal stenosis occurs mainly in older patients due to age related conditions; osteoarthritis of the spine, enlargement of the facet joints, chronic inflammation of the facet joint tissue, bone spurs, herniated or bulging discs and spondylolisthesis. All of these
Lumbar laminectomy means removal of part or all of the lamina at one or more levels of the spine. A lamina is the back or posterior portion of the bone of the spinal canal. This is a slightly more extensive de-compressive procedure than for a lumbar microdiscectomy. A rhizolysis means decompression of the spinal nerves.
With advancing age, and a gradual collapsing of the discs, the lumbar canal narrows due to a combination of thickened ligament and a thickening of the facet joint capsules at the two sides of the spinal column. Patients normally present with pain, weakness and numbness or tingling in one, or both legs. Typically, these symptoms come on while walking.
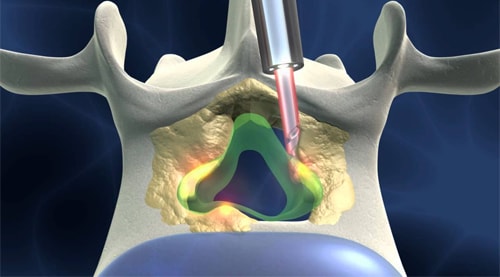
Complete laminectomies almost never need to be performed today. Removing portions of the lamina is known as a full laminectomy, a hemi laminectomy, a partial hemi laminectomy or a foraminotomy. Generally, these procedures can be performed through the same small incision as the microdiscectomy. This causes less disruption to the muscles that attach to the spine. The most common reason for performing a laminectomy, or a partial laminectomy, is to decompress nerves that are compressed by overgrown arthritic bone or cartilage in the lumbar spine. This condition is called lumbar canal stenosis.
Patients normally go home three to five days after surgery and are usually mobile the day after surgery. The post-operative exercise program is the same as for a lumbar microdiscectomy.
Old style laminectomies tended to cause significant back pain after the operation as a large amount of the normal muscular and bone elements had been removed. Today, minimally invasive techniques allow safe and effective decompression of the bone in virtually all cases.
If only the lamina were removed, sometimes the underlying nerve roots may remain compressed. To adequately decompress the nerve roots it may be necessary to remove a portion of the facet joint. This is known as medial facetectomy.
Because of the telescoping and collapsing of the spine as we age, the ligaments between our bones often buckle and cause compression as well. These ligaments may also need to be removed. The subsequent decompression of the nerve root is known in surgical terms as a rhizolysis.
This is the most commonly performed spine operation. It means removing the portion of a disc that has prolapsed and is compressing a nerve. It is performed for sciatica that has not resolved with time or for severe nerve compression due to a large or strategically placed disc protrusion. It is performed using a microscope or an endoscope to minimise disruption to the normal tissues when exposing the disc and nerve.
At the same time as removing the disc fragment, some of the nucleus may be removed. This is referred to as an internal discectomy. In either case most of the disc material is left intact.
After a subtotal discectomy, the disc space will collapse if something is not put in its place. The disc needs to be replaced with either bone or a device that holds the disc space open, such as a cage, disc spacer or an artificial disc.

Following lumbar microdiscectomy, when pressure is taken off a nerve the first symptom to improve is pain. This may be immediate, but it may take longer for the muscle weakness to improve.
If there has been muscle wasting (loss of muscle bulk), this may take up to 3 months to improve. The muscle may never recover its normal muscle bulk if the nerve compression has gone on too long or been too severe.
Any loss of sensation usually recovers quickly, but if the pressure has been severe it may take months to fully recover.
You are encouraged to be mobile the day after surgery for short periods. Do not sit up for long periods, i.e. more than one hour in the first 2 weeks. This is to minimise the risk of recurrent disc prolapse.
You should avoid heavy exercise and heavy lifting for the first six weeks after surgery. Walking is encouraged after 2 weeks following the surgery. Six weeks after your operation you should be walking twice daily for 45 minutes without difficulty.
Subcutaneous stitching is used to approximate the skin following the surgery. There are usually no stitches to remove; the stitch material is buried beneath the skin and will dissolve with time. The wound should be covered for the first five days after the surgery. No dressing is necessary after 5 days.
It is important not to leave a wet dressing on the wound or soak the wound in a bath or swimming pool for more than 30 minutes during the first two weeks after the operation.
After surgery it is not uncommon to have mild lower back pain around the wound. This will improve in the first six weeks following the surgery.
In the first three weeks you may experience mild sciatic pain because of inflammation within the nerve. This usually responds to simple anti-inflammatory drugs. Occasionally, a short course of oral dexamethasone (a strong anti-inflammatory steroid medication) can help reduce the nerve swelling.
You will return for a review at six weeks, at which time you can recommence your normal exercise program.